

There is a lot of confusion about boosters these days. Which one? When? Should I wait for the ‘best’ one? Should I bother? We took a deep dive to try to answer these questions. While we aren’t immunologists, we are skilled at reviewing the literature, and have combined decades of experience in understanding and making recommendations about vaccines of all kinds, for people from infants to seniors.
I don’t have time to read all this, just give it to me straight and simple:
- Vaccines offer insurance against severe outcomes and Long Covid.
- Get boosted as soon as you are eligible.
- Wait at least two months after an infection.
- Vaccines alone, or combined with prior infection, are not enough to prevent infection and reinfection.
- Vaccines alone, or combined with prior infection, are not enough to prevent infection and reinfection. (We thought we should repeat this.)
- We favour a bivalent vaccine, to broaden our immunity beyond the original strain. BA.1 or BA.4-BA.5 bivalent? At this time, there is no clear winner.
- Don’t drop your guard: “there is no such thing as mild Covid.” Dr. Sunny Rae,
Cardiologist, Long Covid Research Clinician @Sunny_Rae1
- Don’t get Covid to not get Long Covid.
- Layer up: "wear an N95 mask, ventilate and filter the air, and avoid the "three Cs" - “Close Contact, Crowded Places, and Closed Spaces."
Immune response: a focus on the Adaptive Immunity
Adaptive Immunity includes both humoral or antibody immunity and cellular immunity.
Part 1: Antibody immunity also called humoral immunity.
When we are vaccinated, we develop antibodies to the protein or antigen used in the vaccine. In the case of COVID, we develop antibodies to the spike protein. The antibodies we form do not stick around in our blood stream. Otherwise, you could well imagine how clogged up our circulation would be with all the antibodies we’ve developed over a lifetime...
When we are exposed to SARS-CoV-2 virus, our immune system recognizes the spike protein from prior vaccination (or infection) and our B lymphocytes produce antibodies to neutralize the spike protein and prevent the virus from entering our cells. Unfortunately, with SARS-CoV-2, the vaccine’s protection has not provided lasting antibody memory, and so over time, the antibodies we produce to stop the virus in its tracks are less and less, and so we get infected.
The booster is a memory jolt telling our B lymphocytes (memory B cells) to make more antibodies. One tricky thing is that the original vaccine was based on the original (or ancestral) strain of SARS-CoV-2, yet with each variant there are mutations in the spike protein, and so the match between the antibodies produced by having been vaccinated (or infected with a previous strain) are not as good a match anymore and are less effective in stopping the virus before an infection sets in.
Tweaking the vaccine to include the newer variant spike protein in the new recombinant vaccine means our bodies will do a better job of recognizing and neutralizing the virus.
Part 2: Cellular immunity, the part responsible for protection against severe COVID-19 outcomes.
Even if our neutralizing antibodies wane over time, our cellular immunity has held up better and for longer, protecting us against severe outcomes (hospitalization, ICU admission, death and possibly decreasing the risk of Long Covid) when we get infected. Cellular immunity includes the B lymphocytes (or antibody producing memory B cells), our T lymphocytes and macrophages, both of which target infected cells.
Only two vaccine doses so far? Get your 3rd dose now!
The arrival of Delta and particularly Omicron, made it clear that to be fully vaccinated against COVID-19, you need three doses. In BC, we still have 1.3 million eligible adults who only have their primary series and have not yet received their third dose, putting them at higher risk of infection and adverse outcomes than those with 1 or 2 booster doses.
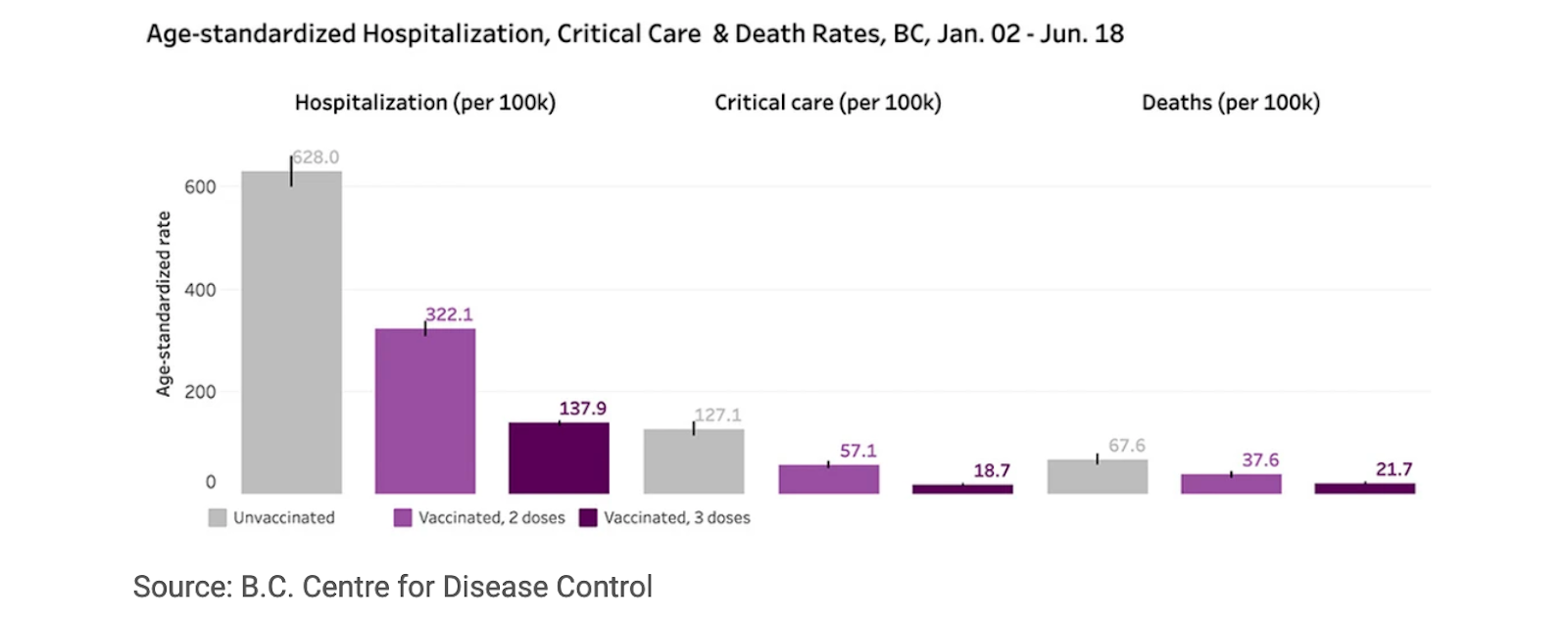
As BC learned during the Delta wave, the elderly (and high risk clinically extremely vulnerable) who may not make as much and as lasting an antibody response to the vaccine, need more frequent boosters to avoid infections and severe outcomes.
The latest US CDC graph up to July 30, 2022, shows that the over 50 years old population also benefits from more boosters.
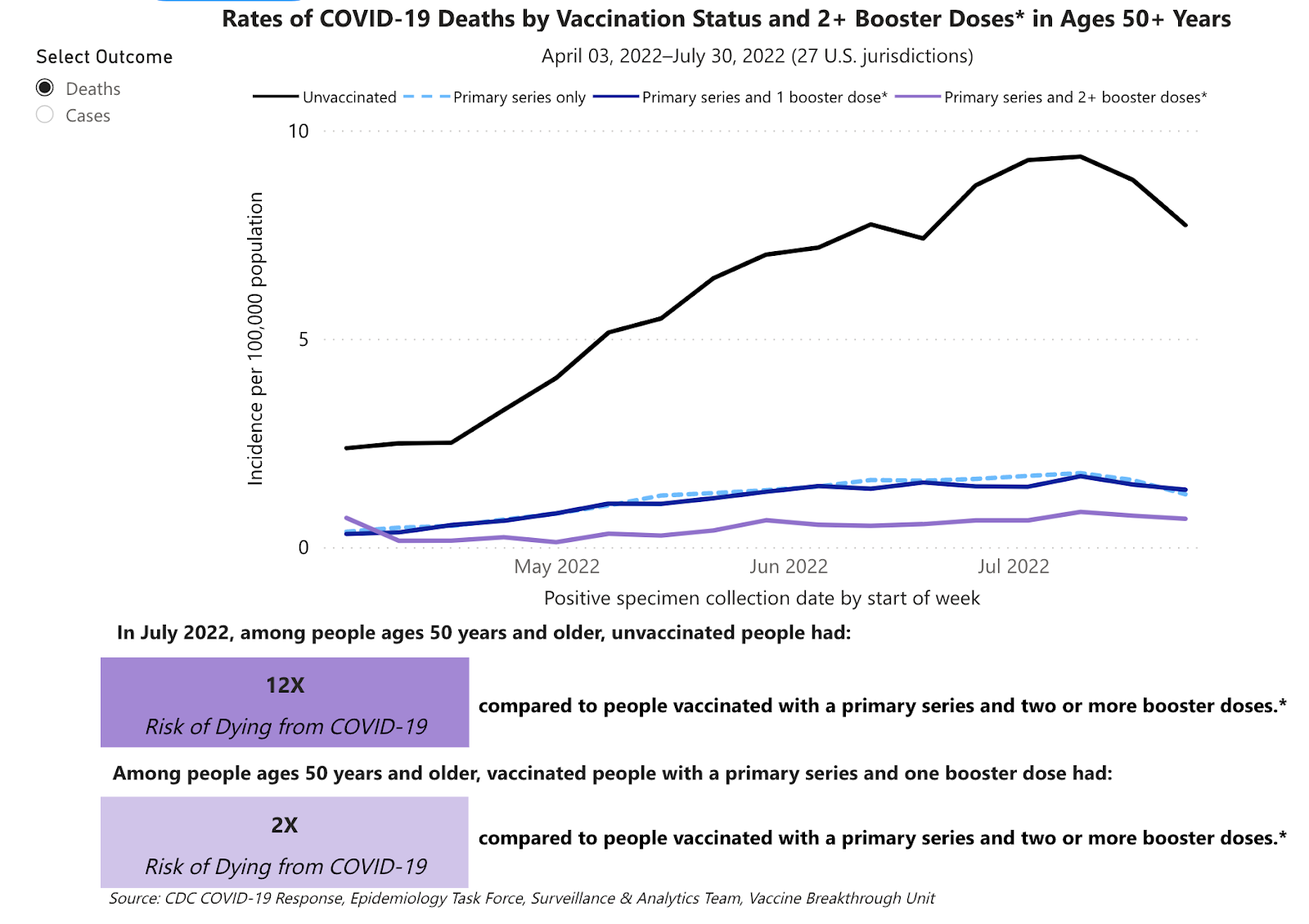
Source: https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status
Last spring, BC had the strictest age-based 4th dose roll out of any province, 70 +, thereby choosing to ration vaccines as they were set to expire. Last July, Protect Our Province BC called on BC Public Health to release the 4th dose to everyone 12 years and over. How well did the 70 + age cutoff for 4th vaccine dose serve British Columbians and limit the stress on our already strained healthcare system?
Ref. Covid weekly report 09-15-2022
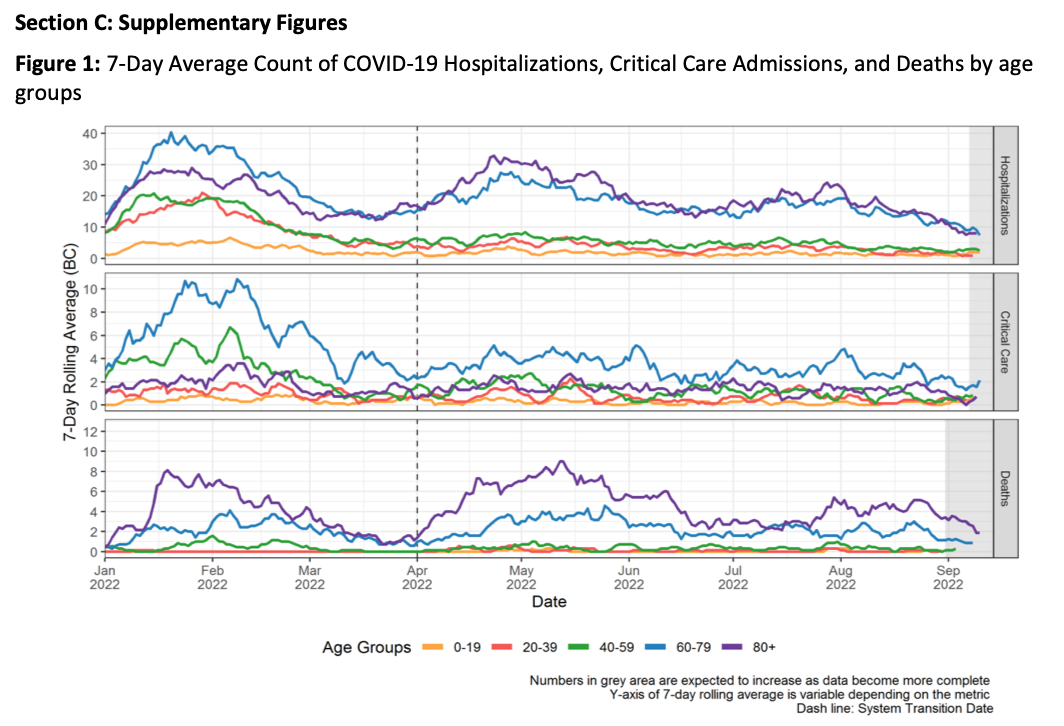
As of September 10th, the 60-69 year olds had 2,164 hospital admissions in 2022, contrast this with 3,142 admissions for the 70-79 year olds during the same period. However when we look at critical care admissions for the 60-69 year olds vs the 70-79, they are the same 715 vs 720 respectively. How many of these ICU admissions could have been avoided with more accessible 4th dose vaccination? How many deaths and grief could have been prevented?
This trend has been obvious for some time now, begs the question why BC Public Health waited until September to at the very least include the over 60 in the age-based roll out for booster priority: Saving vials over Saving Lives?
What about the bivalent booster?
In Canada, the Public Health Agency of Canada, has approved Moderna Spikevax Bivalent, a 50 mcg dose with half being from the original virus and the other half, Omicron BA.1. The National Advisory Committee on Immunization (NACI), recommends this booster for everyone 18 years and over. For the 12-17 year olds who are “moderately to severely immunocompromised” and/or at high risk of severe COVID-19 outcomes because of “biological or social factors”, NACI states the bivalent booster “may be offered off-label.” (Discretionary Recommendation) This may change when Pfizer’s bivalent vaccine gets approved in Canada.
Both the UK and Australia are also rolling out the same Moderna Spikevax Bivalent. The recently published New England Journal of Medicine article outlines the antibody response to the bivalent mRNA-1273.214 vs the original mRNA-1273 Moderna booster as a second booster following a 2 dose-primary Moderna mRNA series and a first booster.
What we know…
Higher levels of neutralizing antibodies against the spike protein offer better protection against infection. We do not know what is the level of neutralizing antibodies needed to achieve protection against infection and severe outcomes with the current circulating variant nor the new ones yet to come.
The NEJM study is based on Moderna’s data and does not provide us with information beyond 29 days post second booster with the bivalent BA.1 vaccine. The study also does not address the strength of the cellular immunity after receiving this booster. More importantly, the study is not a vaccine effectiveness study, it does not answer how many infections with current (and future) circulating variants are avoided by receiving a second booster with the BA.1 bivalent vaccine.
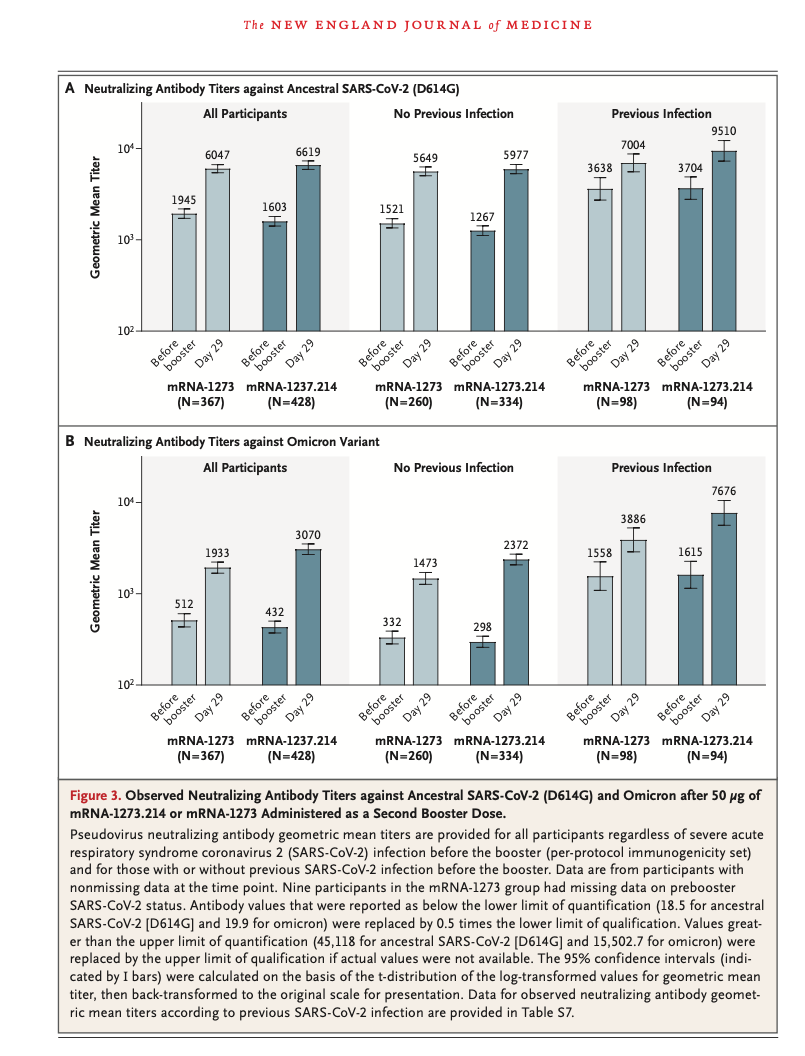
Panel A, Figure 3.: The antibody response to the ancestral SARS-CoV2 (D614G) at 29 days is roughly similar in both immunization groups (original Moderna booster and new bivalent BA.1 booster), though in people with prior COVID infection, the antibody response is greater with the new bivalent booster than the original booster. Note also the greater antibody response in vaccinated individuals with prior infection vs those vaccinated without any prior infection.
This enhanced antibody response to the ancestral strain is what the BC CDC refers to as “hybrid immunity,” from vaccination plus infection. Note that getting infected comes with risk of Long Covid and new health conditions, from immune dysregulation, to diabetes, blood clots, cardiovascular disease and renal dysfunction. As well, “milder” Omicron infections result in “lower antibody titers'' and limited cross-neutralizing immunity between variants, opening the door to reinfection from future variants. So a BA.1 infection does not necessarily protect you from a BA.2 infection nor a new BA.4 infection or BA.5 and so forth.
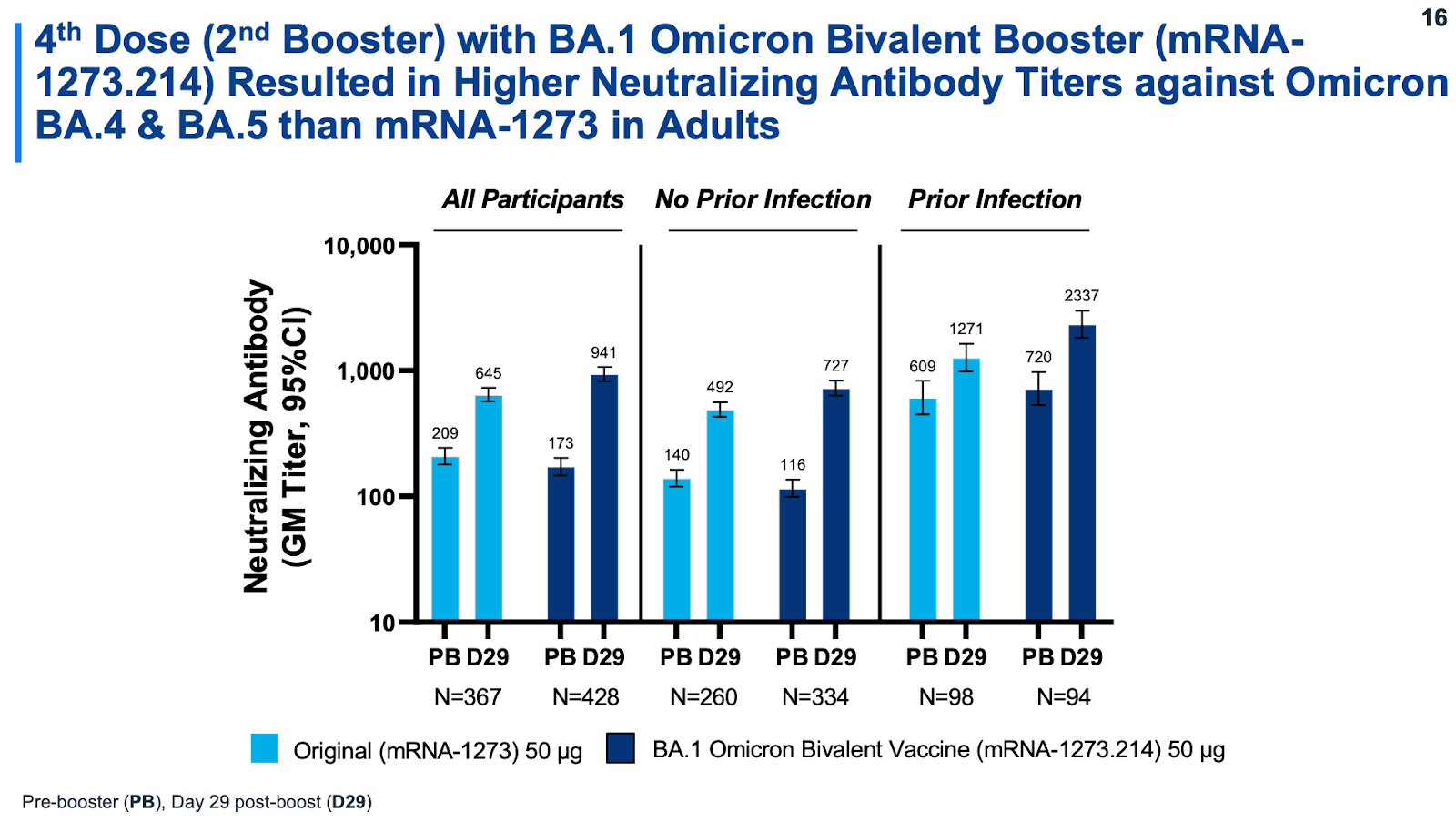
Panel B, Figure 3. : Here you see the antibody response to Omicron after a second original Moderna booster and the newer bivalent booster. The bivalent booster produces a stronger antibody response than the original booster though a much smaller response than that with the ancestral strain. This is partly a result of immune imprinting, where repeated vaccinations against the original virus, plus or minus infection, have led to enhanced B cell memory and their rapid increased production of neutralizing antibodies to the original strain, even after exposure to BA.1 strain.
Immune Imprinting is a bit like a factory production line that keeps on making Blackberry cellphone parts, because that’s what we’ve done over and over and then, even when new cell phones are taking over, the factory fails to shift its production line to Apple cell phone parts. Initially some Blackberry parts (original antibody) are useful in the Apple cell phone but in IOS version 12 (Omicron BA.5 and more) they may no longer be useful.
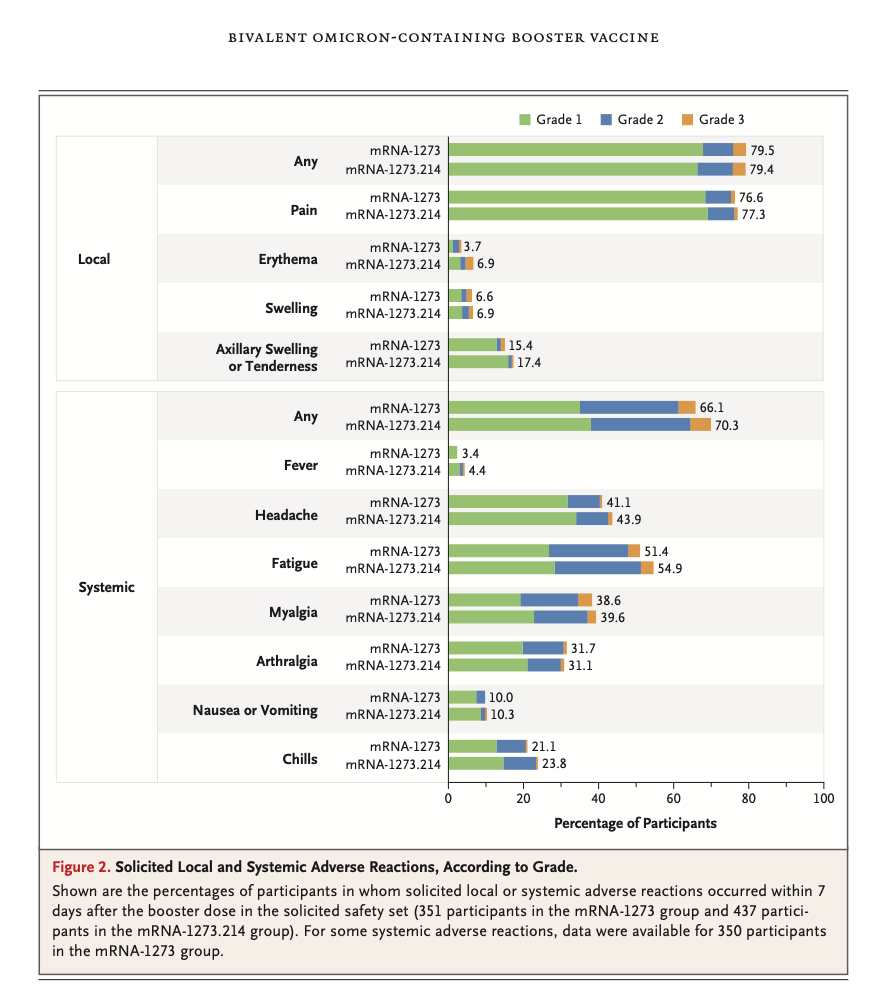
How safe is the new BA.1 bivalent booster vs prior booster?
It is safe. The occurrence of solicited adverse events within 7 days were very similar between the two boosters. Median follow-up was 43 days for the new bivalent booster and 57 days for the original Moderna booster, with no significant differences. No deaths, no myocarditis or pericarditis occurred by the data-cutoff date.
Should you go to the US and get the BA.5-4 bivalent/ ancestral strain booster?
There is no human data available yet for this bivalent vaccine. The FDA approved it based on data from the BA.1 bivalent vaccine and a study in mice. Results from human studies are expected soon.
Note that both the original booster and the BA.1 bivalent booster do elicit neutralizing antibody titers against BA.4 and BA.5, though much fewer than were generated against BA.1 and fewer still than the amount generated by exposure to the ancestral strain (Figure 3 above).
Source: Advisory Committee On Immunization Practice (USA), September 1, 2022 Presentation by Dr. Jacqueline Miller .
Though it may seem like a bivalent vaccine with Omicron BA.4 and BA.5 combination would be more timely than one using the BA.1, the SARS-CoV-2 virus has not finished acquiring new mutations. Chasing newer variants via vaccination is unlikely to work.
“Power of vaccines is directly related to limiting transmission itself.” @yaneerbaryam Complex Systems Physicist, President of @NECSI
Even with newer bivalent vaccines, if we allow mutations to continue unchecked by not making any attempts to control SARS-CoV-2 transmission and sharing vaccines with the world, it will only be a matter of time before our vaccines fail.
https://www.nejm.org/doi/full/10.1056/NEJMra2206573
https://yourlocalepidemiologist.substack.com/p/original-antigenic-sin-are-boosters
https://doi.org/10.1016/j.jinf.2022.09.004





